P1) Non-bilious vomiting in an infant
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with vomiting.
- Review the DDx considerations in a patient with vomiting.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with vomiting.
History
Physical Exam
Labs
Provisional Diagnosis
Potential Acuity
What is your assessment of the likely acuity for this patient?
First Imaging Study
What is the first imaging study you will order?
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
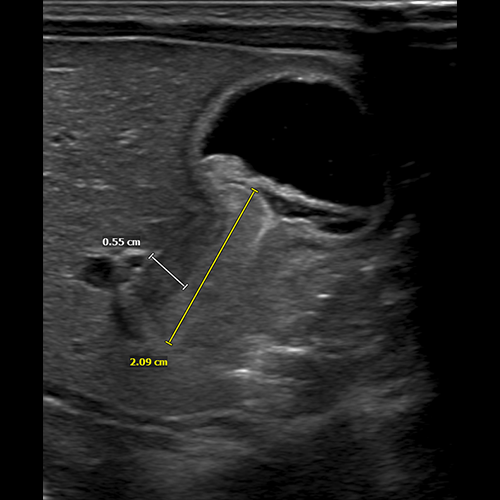
Abdominal ultrasound
What best describes the findings on the abdominal ultrasound?
The length of the pylorus is abnormally increased.
The thickness of the pyloric wall is abnormally increased.

Watch our video
Second Imaging Study
What is the next imaging study you will order?
What is your Diagnosis now that you have seen the imaging results?
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
Assessment and Plan
Please provide your assessment and plan for this patient
Lessons Learned:
- Pyloric stenosis is more likely to occur in preterm male, first-born children who were treated with erythromycin and with a mother who smoked during pregnancy. These factors are all individually associated with increased risk.
- The diagnosis should be suspected in a baby between 2-8 weeks of age presenting with non-bilious vomiting immediately after feeding.
- The first best diagnostic modality is an abdominal ultrasound and reveals and elongated (>12mm) and thickened (>3mm) pylorus. X-ray may suggest gastric outlet obstruction stomach distension.
Socioeconomic Factors: Patients with lower socioeconomic status and who are formula-fed have increased incidence of pyloric stenosis.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Bayar Batmunh, MS - Coordinator

{kind=link}